Adult: Preparations available:
Perindopril arginine 3.5 mg and amlodipine 2.5 mg
Perindopril arginine 7 mg and amlodipine 5 mg
Perindopril arginine 14 mg and amlodipine 10 mg
Perindopril arginine 5 mg and amlodipine 5 mg
Perindopril arginine 5 mg and amlodipine 10 mg
Perindopril arginine 10 mg and amlodipine 5 mg
Perindopril arginine 10 mg and amlodipine 10 mg
Initially, 3.5/2.5 mg once daily. Adjust dosage according to BP goals w/ 7-14 days interval between titrations. Max: Perindopril arginine 14 mg and amlodipine 10 mg once daily. Elderly: Initiate at 2.5 mg amlodipine component once daily.
Adult: Preparations available:
Perindopril erbumine 4 mg and amlodipine 5 mg
Perindopril erbumine 8 mg and amlodipine 5 mg
Perindopril erbumine 4 mg and amlodipine 10 mg
Perindopril erbumine 8 mg and amlodipine 10 mg
As substitution therapy in patients already maintained w/ amlodipine and perindopril: One tab once daily, preferably in the morning.
Renal Impairment
Hypertension: Mild to moderate: Max: Perindopril arginine 7 mg and amlodipine 5 mg. Severe: Not recommended.
Administration
Should be taken on an empty stomach.
Contraindications
History of idiopathic angioedema. Severe hypotension, shock (e.g. cardiogenic shock), left ventricular outflow tract obstruction (e.g. high grade aortic stenosis), heart failure after acute MI. Pregnancy and lactation. Concomitant use w/ aliskiren esp in patients w/ DM or renal impairment (GFR <30 mL/min/1.73 m2).
Special Precautions
Patient w/ salt or volume depletion, severe obstructive coronary artery disease, renal artery and mitral and severe aortic stenosis, ischemic heart disease or cerebrovascular disease, hypertrophic cardiomyopathy w/ outflow tract obstruction, cardiac failure, collagen vascular disease. Hepatic and renal impairment. Elderly. Patient undergoing major surgery or during anaesthesia; desensitisation treatment (e.g. hymenoptera venom).
This drug may cause occasional dizziness or weariness, if affected, do not drive or operate machinery.
Monitoring Parameters
Monitor BP, renal function, electrolytes (e.g. serum K level), CBC w/ differential. Assess cardiac status and fluid balance.
Drug Interactions
Increased hypotensive effects w/ antihypertensive agents (e.g. β-blockers), diuretics, and vasodilators. May increase serum levels and toxicity of lithium. May cause nitritoid reactions w/ Na aurothiomalate. Increased risk of angioneurotic oedema w/ estramustine. May increase hypoglycaemic effect w/ insulin or sulfonamides. Increased antihypertensive effect and risk of orthostatic hypotension w/ TCAs, antipsychotics, anaesthetics, α-blockers. May increase risk of angioedema w/ mammalian target of rapamycin (mTOR) inhibitors (e.g. sirolimus, everolimus, temsirolimus). May cause worsening of renal function and loss of antihypertensive effect w/ NSAIDs. Decreased antihypertensive effects w/ NSAIDs and sympathomimetics.
Amlodipine:
Increased serum concentration of simvastatin. Increased antihypertensive effects w/ amifostine, baclofen. Increased serum concentration w/ CYP3A4 inhibitors (e.g. diltiazem). Decreased serum concentration w/ CYP3A4 inducers (e.g. anticonvulsant agents, rifampicin).
Perindopril:
Increased risk of hyperkalaemia w/ K-sparing diuretics (e.g. amiloride, eplerenone, spironolactone, triamterene), K supplements or other agents which increases serum K level (e.g. NSAID, ciclosporin, heparin, indomethacin). Potentially Fatal: May cause anaphylactoid reactions w/ dextran sulfate in LDL apheresis. May increase risk of hypotension, hyperkalaemia, and changes in renal function w/ aliskiren.
Food Interaction
Food may decrease rate of absorption.
Action
Description: Perindopril, a prodrug of perindoprilat, is an ACE inhibitor which prevents convertion of angiotensin I to angiotensin II, thereby increasing plasma renin activity and decreasing vasoconstriction and aldosterone secretion.
Amlodipine, a dihydropyridine Ca channel blocker, inhibits transmembrane influx of Ca ions into vascular smooth muscle and cardiac muscle thereby causing relaxation and vasodilation. It also directly acts on vascular smooth muscle causing reductions in peripheral vascular resistance and BP. Pharmacokinetics: Absorption: Perindopril: Rapidly absorbed from the GI tract. Effect of food: Slightly reduced absorption w/ food. Absolute bioavailability: Approx 65-75% (perindopril); approx 25% (perindoprilat). Time to peak plasma concentration: 1 hr; 3-4 hr (perindoprilat).
Amlodipine: Well absorbed. Absolute bioavailability: 64-80%. Time to peak plasma concentration: 6-12 hr. Distribution: Perindopril: Volume of distribution: Approx 0.2 L/kg (perindoprilat). Plasma protein binding: 60% (perindopril); 10-20% (perindoprilat).
Amlodipine: Enters breast milk. Volume of distribution: Approx 21 L/kg. Plasma protein binding: Approx 98%. Metabolism: Perindopril: Extensively metabolised in the liver via hydrolysis by hepatic esterases to perindoprilat (as active metabolite) and inactive metabolites including glucuronides.
Amlodipine: Extensively metabolised in the liver to inactive metabolites. Excretion: Perindopril: Via urine (4-12% as unchanged drug). Elimination half-life: 25-30 hr or longer (perindoprilat).
Amlodipine: Via urine (60%, 10% as unchanged drug). Terminal elimination half-life: 30-50 hr.
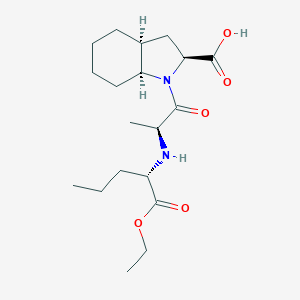
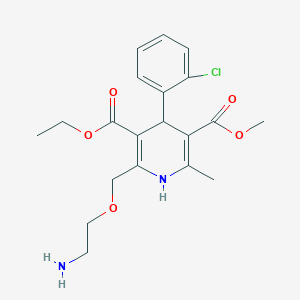
Chemical Structure
Perindopril Source: National Center for Biotechnology Information. PubChem Database. Perindopril, CID=107807, https://pubchem.ncbi.nlm.nih.gov/compound/Perindopril (accessed on Jan. 22, 2020)
Amlodipine Source: National Center for Biotechnology Information. PubChem Database. Amlodipine, CID=2162, https://pubchem.ncbi.nlm.nih.gov/compound/Amlodipine (accessed on Jan. 20, 2020)
Storage
Store below 25°C. Protect from light and moisture.
C09BB04 - perindopril and amlodipine ; Belongs to the class of ACE inhibitors and calcium channel blockers. Used in the treatment of cardiovascular diseases.
References
Anon. Perindopril and Amlodipine. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 01/08/2017.Buckingham R (ed). Amlodipine. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 01/08/2017.Buckingham R (ed). Perindopril. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 01/08/2017.Prestalia (Symplmed Pharmaceuticals, LLC). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/. Accessed 01/08/2017.



 Sign Out
Sign Out